Healthcare Document Processing: Best Tools & Solutions 2026
July 09, 2026
5 min read
Sai S
Last updated July 2026
We have sat across from enough healthcare operations leaders to recognize the same complaint before they finish the sentence. A generic document processing tool clears the demo, gets purchased, and within a quarter the team is back to keying data by hand because the tool never learned to read a faxed referral or a handwritten chart note. Healthcare document processing keeps failing the same way, not because the technology is weak, but because it gets evaluated on the wrong criteria.
The reasons are structural, not incidental. As of 2025, 35% of inbound documents to hospitals and healthcare facilities still arrive by fax, an estimated 80% of clinical data has no fixed schema, and every document sits behind PHI rules, medical code sets, and EHR write-back requirements a generic OCR tool was never built to clear.
There are eight criteria a document processing tool has to clear before it belongs on a healthcare shortlist, and we graded 18 tools against every one of them, organized by the queue each tool actually clears. By the end, you will have a defensible, healthcare-grounded shortlist of two or three vendors matched to your intake channels and team shape, plus a scorecard built to pressure-test any demo before you sign.
Quick Digest
Why healthcare is harder: intake is still fax-dominated (35% of inbound documents), an estimated 80% of clinical data is unstructured, and every document sits behind PHI rules, medical code sets, and EHR write-back requirements.
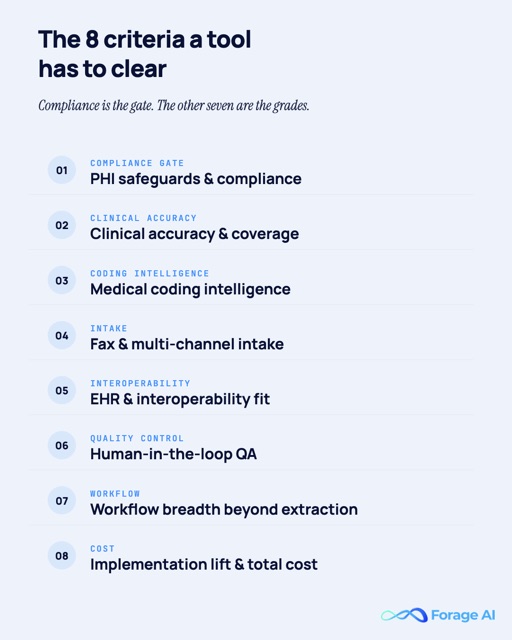
The 8 criteria: PHI safeguards, clinical document accuracy, medical coding intelligence, fax-first intake, EHR fit, human-in-the-loop QA, workflow breadth, and honest implementation cost. Compliance is the gate; the other seven are the grades.
The 18 tools: mapped across 7 categories, from managed done-for-you (Forage AI, #1) to cloud building blocks, each graded on the same rubric.
Fax and intake picks: Tennr for referral-heavy specialty operations, Medsender for clinic-scale fax-to-chart filing, Documo for visible pricing, Consensus for enterprise HITRUST scale.
RCM and prior auth picks: Waystar (+Iodine) for health-system revenue cycle, Infinx for KLAS-top-scored prior authorization automation (90.1/100, April 2026), AGS Health for coding delivered as a service.
Abstraction and IDP picks: Datavant and Reveleer on the payer side; ABBYY, Hyperscience, Nanonets, and Hyland for general IDP with real healthcare depth.
Build vs buy: Reducto and the AWS/Google/Azure stacks are components, not workflows. You own intake, QA, BAA scope, and EHR sync.
How to choose: match the category to your dominant queue, gate by team shape, then make finalists prove field-level accuracy on your own document sample.
Why Is Document Processing Harder in Healthcare Than Anywhere Else?
Start with what actually lands on your desk. Healthcare document processing means capturing the documents that arrive across five queues (the fax inbox, the referral desk, the prior-auth desk, claims intake, and records requests), reading them, and turning them into structured data your systems can act on. The mix is brutal: referrals, CMS-1500 and UB-04 claim forms, clinical notes, lab reports, EOBs, and intake forms, in every format from clean PDFs to handwritten faxes.
Fax is still the front door. Beyond the 35% of inbound documents that arrive by fax, the same 2025 survey of 100+ hospital and clinic administrators and HIM/IT professionals found that 52% of inbound faxes require manual intervention for routing or data extraction, and 88% of practitioners say fax-related delays affect patient care (2025 Healthcare Fax and Workflow Survey, via BusinessWire). Government data published in 2024 shows why fax persists: only 43% of hospitals routinely performed all four interoperability exchange domains as of 2023.
35% of inbound documents to hospitals and healthcare facilities still arrive by fax, and 52% of inbound faxes require manual intervention for routing or data extraction. Source: 2025 Healthcare Fax and Workflow Survey of 100+ hospital and clinic administrators and HIM/IT professionals.
What arrives is mostly unreadable to machines by default. An estimated 80% of clinical data is unstructured, living in free-text notes, scanned documents, and faxes, a figure repeated across NIH-indexed literature as an industry consensus rather than a single measurement. The human cost stacks on top. The AMA‘s newest survey, released May 2026 (fielded December 2025, n=1,000), found physicians complete about 40 prior authorizations per week, consuming 13 hours of physician and staff time weekly, and 94% of physicians link prior auth to burnout (AMA, 2026). Documentation itself eats the clinic day: for a 30-minute primary care visit, physicians spend about 36 minutes in the EHR (Annals of Internal Medicine, 2025, via AMA coverage).
40 prior authorizations per physician per week, consuming 13 hours of physician and staff time; 94% of physicians link prior authorization to burnout. Source: AMA physician survey (n=1,000), released May 2026.
Here is the chain that matters for tool selection: fax-dominated intake, plus unstructured data, plus PHI gates, plus code-set dependence, plus the requirement that extracted data lands back in Epic or Cerner (Oracle Health). Generic OCR and IDP tools underperform against that chain, which is why healthcare document automation gets evaluated on healthcare-specific criteria. One warning from the field first: digitizing faxes alone does not fix intake. Cloud fax without extraction moves the backlog on-screen, which is why document digitization is the start of the work, not the end of it.
Forage AI promotional banner reading your team should not spend the day keying fax packets, with a talk to our expert call to action.
Quick Summary
Q: Why is document processing harder in healthcare than in other industries?
A: Because intake is still fax-dominated (35% of inbound documents as of 2025) and an estimated 80% of clinical data is unstructured, while every document sits behind PHI rules, medical code sets, and EHR write-back requirements that generic tools do not handle. The prior-auth desk alone consumes about 13 hours of physician and staff time per week (AMA, 2026).
Expert Insights
“Physician trust in voluntary insurer pledges is deeply eroded after years of unfulfilled promises. Physicians are especially frustrated when so-called peer-to-peer reviews are conducted by individuals who lack the appropriate clinical expertise to evaluate a patient’s care.”
Bobby Mukkamala, M.D., President, American Medical Association, on the 2026 AMA prior authorization survey, which found 94% of physicians link prior auth to burnout.
What a Healthcare Document Processing Tool Must Have: 8 Evaluation Criteria
Each of healthcare’s document challenges maps to a capability you can test in a demo, and that mapping is the rubric below. One anchor definition first: intelligent document processing (IDP) is software that classifies documents and extracts structured, validated data from them using AI, a different job from OCR’s raw text conversion (our OCR vs IDP explainer draws the line).
Our method is simple to state: we graded every vendor, including ourselves, on the same eight healthcare IDP criteria. No vendor paid for placement.
Referrals, eligibility, PA submission, claims edits, denials
8
Implementation lift & total cost
Tools die in month three of implementation
Honest time-to-live and a pricing model you can explain to finance
Infographic listing the eight healthcare document processing evaluation criteria: PHI safeguards and compliance, clinical accuracy and coverage, medical coding intelligence, fax and multi-channel intake, EHR and interoperability fit, human-in-the-loop QA, workflow breadth beyond extraction, and implementation lift and total cost.
Treat criterion 1 as a gate, not a grade you trade against. The average U.S. healthcare data breach cost $7.42 million in 2025, the costliest of any industry for the 14th consecutive year, and healthcare breaches take the longest to contain at an average of 279 days (IBM Cost of a Data Breach Report, 2025). Accuracy claims deserve equal scrutiny, because extraction errors surface as denials. In Experian Health’s 2025 State of Claims survey, 41% of providers said claims are denied 10% or more of the time, and missing or inaccurate claim data was the #1 cited cause of denials, named by 50% of respondents.
$7.42 million: the average cost of a U.S. healthcare data breach in 2025, the costliest of any industry for the 14th consecutive year. Source: IBM Cost of a Data Breach Report, 2025.
One more distinction is worth ruling out before the roster: a category mix-up shows up constantly in search results for this topic.
Document management software is not document processing software. DMS platforms (the DocuWare and SmartVault class) store and route files; document processing tools read them and extract data. Half the pages ranking for healthcare document management software list storage tools for an extraction job. If the pitch is folders, retention policies, and eSignatures, it belongs in a different evaluation.
Quick Summary
Q: What must a healthcare document processing tool have before it earns a shortlist spot?
A: Eight criteria: PHI safeguards, clinical document accuracy, medical coding intelligence, fax-first intake, EHR fit, human-in-the-loop QA, workflow breadth, and honest implementation cost. Compliance is the gate; the other seven are the grades you compare vendors on.
Expert Insights
“AI is no longer just a theoretical solution, but it’s a vital tool that can break the pervasive cycle of denials, delays, and data errors.”
Clarissa Riggins, Chief Product Officer, Experian Health. Her company’s 2025 State of Claims survey (250 healthcare billing and claims decision-makers) found 41% of providers now see denial rates above 10%, and half trace denials to missing or inaccurate claim data.
The 18 Best Healthcare Document Processing Tools at a Glance
With the eight-criterion rubric set, here is the field. Even Gartner‘s first-ever Magic Quadrant for Intelligent Document Processing Solutions, published September 3, 2025, evaluated 18 vendors in a market of 100+ and named five Leaders, yet it does not segment by healthcare. Nobody has graded this category on healthcare terms. The seven categories below do: each answers a different queue, so find your queue first.
18 vendors, 5 Leaders, zero healthcare segmentation: Gartner published its first-ever Magic Quadrant for Intelligent Document Processing Solutions on September 3, 2025, mapping a market of 100+ vendors without grading any of them on healthcare-specific criteria. Source: Gartner, 2025.
Deliberately not on this list: DMS and storage tools, eSign tools, and generic IDP vendors without a demonstrated healthcare practice (see the DMS-vs-IDP callout under the evaluation criteria).
#
Tool
Category
Best for
1
Forage AI
Managed / done-for-you
Clean, QA’d data delivered without staffing a platform
2
Tennr
Fax & intake automation
Referral-heavy specialty operations (DME, imaging, home health)
3
Medsender
Fax & intake automation
Clinic-scale fax-to-EHR chart filing
4
Documo
Fax & intake automation
Fax transport + extraction with published pricing
5
Consensus Cloud Solutions
Fax & intake automation
Enterprise fax + extraction under one HITRUST roof
6
Waystar (+ Iodine)
RCM / claims / prior auth
Health systems wanting document intelligence inside the revenue cycle
Network-scale chart abstraction for payers and VBC
10
Reveleer
Clinical abstraction
Focused risk adjustment and HEDIS chart review
11
ABBYY
General IDP
Enterprise claims-forms capture with IT capacity
12
Hyperscience
General IDP
Enterprise claims operations with heavy handwriting
13
Nanonets
General IDP
Self-serve IDP with visible pricing and fast setup
14
Hyland (OnBase + IDP)
General IDP
Hospitals already on OnBase
15
Reducto
Developer-first API
AI/platform teams embedding extraction in a product
16
AWS (Textract + Comprehend Medical)
Cloud building blocks
AWS-native engineering teams
17
Google Cloud (Document AI + Healthcare NLP)
Cloud building blocks
Teams wanting trainable parsers on GCP
18
Microsoft Azure (Document Intelligence + Text Analytics for Health)
Cloud building blocks
Microsoft-ecosystem and data-residency-sensitive orgs
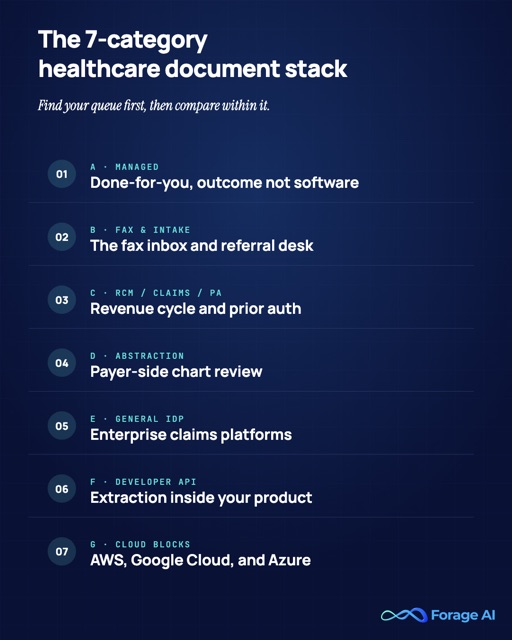
Infographic mapping the seven healthcare document processing categories: managed done-for-you, fax and intake automation, RCM, claims and prior authorization, clinical abstraction, general IDP, developer-first APIs, and cloud building blocks.
Quick Summary
Q: Which healthcare document processing tools are worth shortlisting in 2026?
A: Eighteen tools across seven categories, and the right one depends on your queue: managed done-for-you (Forage AI), fax and intake (Tennr, Medsender, Documo, Consensus), RCM and prior auth (Waystar, Infinx, AGS Health), abstraction (Datavant, Reveleer), general IDP (ABBYY, Hyperscience, Nanonets, Hyland), developer APIs (Reducto), and cloud building blocks (AWS, Google, Azure).
Best Managed, Done-for-You Healthcare Document Processing
Every category after this one hands your team software to run. This category is for the opposite case: you want the output (clean data in your systems), not another platform to staff. Managed document processing earns its slot when there are no engineers to spare and no appetite to hire the QA layer that document processing automation requires.
Strong. Built-in validation, audit trails, and encryption;
Clinical document coverage & accuracy
Excellent. Handwritten notes and low-resolution scans via HDR-enhanced OCR; documents over 2,000 pages; in-house ML with 95% table-detection accuracy.
Medical language & coding intelligence
Adequate. Clinical notes, lab reports, and insurance forms handled; no standalone ICD/CPT inference engine claimed.
Fax & multi-channel intake
Strong. Ingests PDF, DOC/DOCX, EML/MSG, JPG/PNG/TIFF, including faxed and scanned packets; not a fax transport line.
EHR & interoperability fit
Adequate. Delivers to ERP/CRM/databases via secure protocols and webhooks in CSV/JSON/XML; EHR-native HL7/FHIR delivery not asserted here.
Human-in-the-loop QA & exception handling
Excellent. 3x QA team on every delivery; automated checks plus human verification; accuracy tuned via feedback loops.
Workflow breadth beyond extraction
Limited. An extraction and delivery service, not a referral/PA/denials workflow product.
Implementation lift & total cost
Excellent. Onboarding in 1-2 weeks; no engineering burden on your side.
Best for
Teams that want clean, QA’d data landing in their systems without staffing a platform
Pricing model
Managed service (custom scope)
Review signal
n/a: services firm with no G2/KLAS listing; graded on documented evidence, stated transparently
The one entry on this list where you buy the outcome, not the software. Forage AI builds, runs, QA’s, and maintains the extraction pipeline; what reaches your systems is the data. The evidence base: 10M+ documents parsed, an in-house ML model with 95% table-detection accuracy, documents over 2,000 pages handled, and handwritten notes and low-res scans processed through HDR-enhanced OCR. Forage AI delivers the data, not just the pipeline. Healthcare coverage spans clinical notes, lab reports, and insurance forms, plus provider directories through entity matching, adjacent to its healthcare data extraction work.
10M+ documents parsed, with an in-house ML model at 95% table-detection accuracy and documents over 2,000 pages handled. Source: Forage AI, 2026.
The QA posture is the reason this model exists. Every Forage AI delivery passes a 3x QA team before it lands in your system, and pipelines run under HIPAA-compliant workflows with validation, audit trails, and encryption. In one anonymized healthcare provider data engagement, the team reports extracting 1M+ provider profiles across 350K practices, citing 99.7% field-level accuracy on golden-set evaluation and a 90% reduction in the client team’s data collection time (self-reported program results). Onboarding runs 1-2 weeks, and delivery lands in your ERP, CRM, or databases over secure protocols and webhooks. We grade our own EHR criterion conservatively on purpose: chart-native HL7/FHIR write-back is not a claim we make on this page. Details live on the Intelligent Document Processing page.
Who it’s for: operations teams whose faxes, handwritten notes, and 2,000-page records defeat template tools, and who would rather buy the extraction outcome than hire for it. Watch-out: not self-serve software. There is no dashboard your team drives day-to-day and no G2 rating to cite; if you want a tool your own team operates, look at categories B through E.
Quick Summary
Q: When is a managed document processing service the right choice for healthcare teams?
A: When you need the extraction outcome without staffing a platform: no engineers to allocate, no QA team you want to hire, and a document mix (faxes, handwriting, 2,000-page records) that defeats template tools. The tradeoff is that you operate nothing yourself.
Forage AI promotional banner reading get the data, not the software to run, with a talk to our expert call to action.
Best Healthcare-Native Fax and Intake Automation
If the managed model is not your shape, the next question is your loudest queue, and for most provider organizations that is still fax. The interesting 2026 story is that fax is being re-platformed, not retired: AI extraction is being layered onto fax transport. The category exists because digital fax alone solved nothing; 52% of inbound faxes still need manual handling even when they arrive as pixels (2025 Healthcare Fax and Workflow Survey). These four vendors treat HIPAA compliant fax as first-class intake and differ mainly on scale and depth.
2. Tennr
Tennr provider card: healthcare fax and intake automation, about 10 million documents processed per month.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. Healthcare-native platform processing PHI for hundreds of healthcare orgs; confirm BAA scope in diligence.
Clinical document coverage & accuracy
Strong. Purpose-built language models read referral faxes, including messy multi-page packets.
Medical language & coding intelligence
Adequate. Referral and eligibility context, not a coding engine.
Fax & multi-channel intake
Excellent. Fax-first by design; roughly 10M documents/month processed.
EHR & interoperability fit
Strong. Extracts, routes, and pushes work downstream into intake systems.
Excellent. Eligibility checks, benefits investigation, PA submission, and now Voice AI for referral calls.
Implementation lift & total cost
Adequate. Enterprise sales motion; pricing not published.
Best for
Referral-based specialty operations: DME, imaging, home health
Pricing model
Enterprise / custom
Review signal
G2 lists zero reviews for Tennr as of mid-2026; grade on funding and named deployments, not star ratings
The referral desk’s strongest specialist. Tennr’s purpose-built language models read referral faxes, then run the downstream steps that eat staff hours: eligibility, benefits investigation, prior auth submission. It processes roughly 10M documents per month across hundreds of healthcare organizations; a $101M Series C led by IVP in June 2025 brought total funding to about $162M.
The 2026 momentum: a TwelveStone Health Partners partnership (January 2026), expansion into orthopedics, cardiology, and fertility, a first Chief Medical Officer (William Morris, M.D.), and a Voice AI product for referral phone calls. Who it’s for: referral-heavy specialty operations, where named deployments like Norco Inc back the pitch. Watch-out: young company, enterprise pricing opacity, thin review-site volume; grade it on funding and named deployments, not star ratings.
3. Medsender
Medsender provider card: healthcare fax and intake automation, 30 to 40 staff hours saved per week.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. HIPAA-compliant AI fax platform; HIPAA-compliant patient email without portal logins.
Clinical document coverage & accuracy
Strong. AI labels every inbound fax and identifies the right patient.
Medical language & coding intelligence
Limited. Not a coding or clinical NLP product.
Fax & multi-channel intake
Excellent. Fax-first with email and referral-module channels.
EHR & interoperability fit
Strong. Files documents to the correct patient chart in the EHR; reviewers single out the EMR integration.
Human-in-the-loop QA & exception handling
Adequate. Routing review supported; formal exception tooling is lighter than enterprise IDP.
Workflow breadth beyond extraction
Adequate. Referral module and patient communication, not RCM workflows.
Implementation lift & total cost
Strong. SMB-friendly setup; reviewers cite affordability vs other cloud fax.
Best for
Clinics and SMB practices automating fax-to-chart filing
Pricing model
Subscription
Review signal
G2-listed; reviewers consistently praise EMR integration, support, and affordability. A specific star rating could not be independently confirmed at publish
Fax-to-chart filing without enterprise procurement. Medsender’s AI labels every inbound fax and files it to the correct patient chart in the EHR, with a referral module and HIPAA-compliant patient email that skips portal logins. G2 reviewers consistently praise the EMR integration, responsive support, and affordability relative to other cloud fax options.
Vendor-reported but concrete: one dermatology group reports saving 30-40 staff hours per week (vendor case study). Who it’s for: clinics and SMB practices that want fax-to-chart automation this quarter, not after a six-month rollout. Watch-out: SMB heritage cuts both ways; heavy claims and RCM organizations will outgrow it.
4. Documo
Documo provider card: healthcare fax and intake automation, G2 rating 4.6 out of 5 across 190 reviews.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. HIPAA cloud fax with SOC 2; HITRUST-aligned.
Clinical document coverage & accuracy
Adequate. Native IDP layer classifies, extracts, routes; not a clinical NLP stack.
Medical language & coding intelligence
Limited. No medical code-set intelligence claimed.
Fax & multi-channel intake
Excellent. mFax cloud fax core plus extraction on top.
EHR & interoperability fit
Adequate. API-driven delivery; EHR connectivity is integration work.
Human-in-the-loop QA & exception handling
Adequate. Routing and review supported at the platform level.
Workflow breadth beyond extraction
Adequate. Fax workflow plus extraction, not downstream RCM.
Implementation lift & total cost
Strong. Published per-page cloud-fax pricing; developer-friendly API praised in third-party roundups.
Best for
Teams that want fax transport + extraction from one vendor with visible pricing
Pricing model
Per-page cloud fax (published); IDP add-on custom
Review signal
G2: 4.6/5 across 190 reviews (accessed 2026-07-08); developer-friendly API also praised in third-party roundups
The transparent-pricing pick in a category that hides its rate card. Documo pairs HIPAA cloud fax (mFax) with a native IDP layer that classifies, extracts, and routes, under SOC 2 and HITRUST-aligned controls. Published per-page fax pricing is rare here and makes budgeting honest, and third-party roundups repeatedly praise the developer-friendly API. Documo rates 4.6/5 across 190 reviews on G2 (accessed 2026-07-08).
Worth knowing: Documo fielded the 2025 fax survey cited throughout this article. Who it’s for: teams that want transport plus extraction from one vendor and a price they can read before the sales call. Watch-out: it is a fax-first platform; the extraction layer is an add-on, not a full clinical NLP stack.
5. Consensus Cloud Solutions (eFax + Clarity)
Consensus Cloud Solutions provider card: healthcare-native fax and intake automation, HITRUST r2 certification held since 2019.
Criterion
Grade + evidence
PHI safeguards & compliance
Excellent. eFax Corporate has held HITRUST r2 since 2019, re-certified January 27, 2026, the first major cloud-fax provider to do so.
Clinical document coverage & accuracy
Strong. Clarity applies NLP/ML + OCR to faxes, scans, and handwriting.
Medical language & coding intelligence
Adequate. Structured-data output; code-set depth to validate in demos.
Fax & multi-channel intake
Excellent. Enterprise cloud-fax incumbent at national scale.
EHR & interoperability fit
Strong. Unite product bridges fax output into interoperability workflows.
Health systems needing enterprise-scale fax + extraction under one HITRUST roof
Pricing model
Enterprise / custom
Review signal
Clarity has no dedicated G2 listing; the broader Consensus/eFax listing carries 1,700+ G2 reviews, but that figure isn’t Clarity-specific
The enterprise incumbent that added a reading layer. Consensus (NASDAQ: CCSI) runs the eFax Corporate estate, and its Clarity product turns faxes, scans, and handwriting into structured data with an interoperability bridge (Unite) behind it. The compliance posture is the headline: HITRUST r2 held since 2019 and re-certified in January 2026, plus an active healthcare presence through HIMSS 2026.
Who it’s for: health systems that need enterprise-scale fax and extraction under a single, certifiable vendor. Watch-out: the heritage is transport, and Clarity is newer than the fax business; validate extraction depth against your document mix in demos.
Quick Summary
Q: What is the best fax and intake automation software for healthcare?
A: Tennr for referral-heavy specialty operations, Medsender for clinic-scale fax-to-EHR filing, Documo for transparent-pricing fax plus IDP, and Consensus for enterprise HITRUST-certified scale. All four treat fax as first-class intake; they differ on depth, scale, and procurement weight.
Expert Insights
“Patients really shouldn’t vanish into a work queue. There’s so much opportunity to build a delightful patient experience, but it’s always failed because we expect so much behavior change from providers who are completely overwhelmed.”
Trey Holterman, CEO and co-founder, Tennr (June 2025). The customer side of the same story, from Ty Barnett, CIO of Norco Inc: “Tennr has revolutionized our fax-to-intake workflow, eliminating hundreds of hours of manual effort each day, removing human errors, and accelerating the creation of patient intakes.”
Best for Revenue Cycle, Claims, and Prior Authorization
The fax queue is where document pain starts; the PA and claims desk is where it converts to revenue pain. The AMA’s 2026 survey counts roughly 40 prior auths per physician per week, and Experian Health’s 2025 data puts missing or inaccurate claim data as the #1 cause of denials. Prior authorization automation and claims processing automation are therefore where document processing budgets are easiest to defend. Three vendors dominate the shortlists here, each with a different delivery model.
6. Waystar (+ Iodine Software)
Waystar provider card: revenue cycle management, claims, and prior authorization, Best in KLAS 2026 with a score of 98.4.
Strong. Iodine’s AI models are trained on a clinical dataset representing more than a third of U.S. inpatient discharges.
Medical language & coding intelligence
Excellent. Iodine’s CDI engine is the acquisition’s whole point: clinical documentation integrity at hospital scale.
Fax & multi-channel intake
Adequate. Intake is not the platform’s center of gravity.
EHR & interoperability fit
Strong. Revenue-cycle integration across 1M+ providers.
Human-in-the-loop QA & exception handling
Adequate. Workflow review inside the RCM suite.
Workflow breadth beyond extraction
Excellent. Full revenue cycle: claims, denials, payments, now CDI.
Implementation lift & total cost
Limited. An enterprise suite decision, not a point-tool purchase.
Best for
Hospitals and health systems wanting document intelligence embedded in the revenue cycle
Pricing model
Enterprise / custom
Review signal
Best in KLAS 2026 for EHR Revenue Cycle Optimization (score 98.4) and Revenue Cycle: Contract Management (92.4); Best in KLAS for Claims & Clearinghouse every year since 2010
Document intelligence embedded in the revenue cycle, not bolted beside it. Waystar serves about 30,000 clients representing more than 1M providers, and on October 1, 2025 it closed the $1.25B acquisition of Iodine Software. Iodine brings 1,000+ hospital and health-system clients and an AI clinical documentation integrity engine trained on a dataset representing more than a third of U.S. inpatient discharges. The deal resets what claims processing software means at the enterprise end.
Who it’s for: hospitals and health systems that want clinical and financial document intelligence inside the platform that already runs their revenue cycle. Watch-out: overkill for clinics, and the document processing is embedded in the suite; you cannot buy it standalone.
7. Infinx
Infinx provider card: revenue cycle management, claims, and prior authorization, KLAS score 90.1 out of 100 as of April 2026.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. Healthcare-only prior auth and patient access platform.
Clinical document coverage & accuracy
Strong. PA documentation handled end-to-end with AI plus specialists.
Medical language & coding intelligence
Adequate. Patient-access and PA context, not autonomous coding.
Fax & multi-channel intake
Adequate. Intake handled within PA workflows.
EHR & interoperability fit
Strong. Epic marketplace listing reported; verify current status in diligence.
Human-in-the-loop QA & exception handling
Excellent. The product IS an AI + human-in-the-loop hybrid; exceptions route to specialists.
Adequate. Tech + services engagement rather than pure SaaS.
Best for
Provider organizations drowning in PA volume
Pricing model
Enterprise / services hybrid
Review signal
KLAS April 2026: 90.1/100, segment average 85.8; 96% would buy again
The KLAS-scored prior auth specialist. In KLAS Research’s April 2026 Revenue Cycle Prior Authorization report card, Infinx earned the segment’s highest overall score at 90.1/100 against a segment average of 85.8, with 96% of customers saying they would buy again. The model is AI plus human-in-the-loop: automation handles the determinations it can, and specialists absorb the exceptions, which is exactly the shape PA work has.
90.1/100: Infinx earned the highest overall score in KLAS Research’s Revenue Cycle Prior Authorization report card, against a segment average of 85.8; 96% of customers would buy again. Source: KLAS Research, April 2026.
The vendor also claims above-98% auth-determination accuracy (vendor figure; test on your mix). Who it’s for: provider organizations where PA volume, not general document volume, is the fire. Watch-out: it is a PA and patient-access specialist rather than a general document processor, and the services component means part of what you buy is BPO.
8. AGS Health
AGS Health provider card: revenue cycle management, claims, and prior authorization, 500-plus digital agents in production.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. Established RCM services provider operating on PHI at scale.
Clinical document coverage & accuracy
Strong. Coding-grade document reading across clinical and billing docs.
Medical language & coding intelligence
Excellent. Autonomous coding and computer-assisted coding across ICD/CPT.
Fax & multi-channel intake
Strong. UiPath AI25 award won specifically for healthcare fax-intake automation.
EHR & interoperability fit
Adequate. Works within client systems as a service.
Human-in-the-loop QA & exception handling
Excellent. Human review is native to the services model.
Workflow breadth beyond extraction
Excellent. Full RCM: coding, billing, denials, AR.
Implementation lift & total cost
Adequate. A services engagement, not a software install.
Best for
Organizations that want coding/RCM outcomes delivered as a service at offshore scale
Pricing model
Managed services
Review signal
2021 Best in KLAS for Outsourced Coding; named Most Improved Services Solution in KLAS’s 2024 Best in KLAS Software & Services report (14% year-over-year client satisfaction gain)
Coding outcomes as a service, with automation underneath. AGS Health pairs RCM services with its Intelligent RCM Engine: autonomous coding and computer-assisted coding across ICD and CPT, with 500+ digital agents in production. Its fax-intake automation won a UiPath AI25 award, a useful third-party signal in a category full of self-graded homework.
Who it’s for: organizations that want medical coding automation and RCM outcomes delivered at offshore scale without building the capability internally. Watch-out: this is an RCM outsourcer with AI, not software you license standalone; if you want a tool your team runs, look at category E.
Quick Summary
Q: Which tools automate claims and prior authorization document work best?
A: Waystar (with Iodine) for health-system revenue cycle with embedded clinical intelligence, Infinx for prior authorization (the segment’s top KLAS score, 90.1/100 in April 2026), and AGS Health for coding and RCM outcomes delivered as a service. All three are provider-side plays with different delivery models.
Expert Insights
“Iodine joining Waystar brings together comprehensive clinical and financial intelligence on a single AI-powered platform,”
said Waystar CEO Matt Hawkins at the deal’s close (October 2025), calling the combination a unique differentiator in the market. A $1.25B price for a CDI engine says document intelligence is becoming revenue-cycle infrastructure, not an add-on.
Best for Clinical Data Abstraction and Record Review
Everything so far clears intake queues. Clinical data abstraction is document processing at a different altitude: reading longitudinal charts for risk adjustment coding, HEDIS quality, and medical record review, mostly on the payer and value-based care side. If your queues are front-office, skip this category; if you carry risk, it is the whole game.
9. Datavant
Datavant provider card: clinical abstraction, 60 million-plus records connected across 80,000-plus facilities.
Criterion
Grade + evidence
PHI safeguards & compliance
Excellent. Privacy-protected health data exchange is the core business.
Clinical document coverage & accuracy
Strong. NLP/AI over unstructured longitudinal charts (Clinical Insights Platform, launched March 2025).
Medical language & coding intelligence
Strong. Risk adjustment, payment integrity, and quality use cases.
Fax & multi-channel intake
Limited. Not an intake tool.
EHR & interoperability fit
Strong. Network connectivity spanning 80,000+ hospitals and clinics.
Human-in-the-loop QA & exception handling
Adequate. Abstraction review workflows; public detail limited.
Workflow breadth beyond extraction
Strong. Record retrieval, abstraction, real-world evidence (Aetion).
Implementation lift & total cost
Limited. Network-scale enterprise engagement.
Best for
Payers and risk-bearing providers doing VBC chart work at network scale
Pricing model
Enterprise / custom
Review signal
2026 Best in KLAS winner for Risk Adjustment: Coding, Retrieval & Compliance Solutions (90.5/100) and for Outsourced Coding (94.9/100 vs. 88.4 category average); not meaningfully covered on G2
Abstraction at network scale. Datavant’s exchange network moves 60M+ healthcare records between thousands of organizations, spanning 80,000+ hospitals and clinics, 75% of the 100 largest health systems, and 300+ real-world data partners. On top of that network it has stacked abstraction capability fast: Apixio’s VBC platform absorbed in September 2024, the Clinical Insights Platform launched March 2025, and the ~$400M acquisition of RWE platform Aetion completed July 11, 2025.
60M+ records moved across 80,000+ hospitals and clinics: Datavant’s exchange network spans 75% of the 100 largest health systems and 300+ real-world data partners. Source: Datavant, 2025.
Who it’s for: payers and risk-bearing providers doing risk adjustment and quality chart work where record access at scale is half the battle. Watch-out: it is payer/VBC-oriented rather than an intake tool, and the Apixio brand sunset can confuse a buying committee mid-evaluation; confirm which platform name you are actually contracting for.
10. Reveleer
Reveleer provider card: clinical abstraction, KLAS risk-adjustment score of 75.0.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. Payer-grade risk adjustment and quality platform.
Clinical document coverage & accuracy
Strong. AI chart abstraction across retrieved records.
Medical language & coding intelligence
Strong. Risk adjustment and HEDIS-focused extraction.
Fax & multi-channel intake
Limited. Not an intake product.
EHR & interoperability fit
Adequate. Pre-encounter clinical data aggregation via the MDPortals lineage.
Human-in-the-loop QA & exception handling
Adequate. Abstraction review built into the workflow.
Workflow breadth beyond extraction
Adequate. Risk adjustment, quality, member management.
Implementation lift & total cost
Adequate. Focused platform, lighter than a network play.
Best for
Health plans and risk-bearing groups wanting focused abstraction
Pricing model
Enterprise / custom
Review signal
KLAS gives the Reveleer Risk Adjustment Solution a 75.0 overall performance score; no G2 listing found
The focused alternative to a network play. Reveleer does AI chart abstraction for risk adjustment, HEDIS quality, and member management, with clinical data aggregation and pre-encounter intelligence lineage from its 2023 MDPortals acquisition. Where Datavant sells the network, Reveleer sells the abstraction workbench.
Who it’s for: health plans and risk-bearing provider groups that want a dedicated abstraction platform without contracting for a data network. Watch-out: it is a payer-side platform; if your pain is the front-office fax and referral queue, nothing here touches it.
Quick Summary
Q: What are the best tools for clinical data abstraction and medical record review?
A: Datavant for network-scale abstraction (60M+ records moved, 80,000+ facilities, plus the 2025 Clinical Insights Platform) and Reveleer for focused risk-adjustment and HEDIS chart review. Both are payer and VBC plays, not intake automation.
Best General IDP Platforms With Real Healthcare Depth
Now the horizontal platforms, with a healthcare filter applied hard. This is the category Gartner’s inaugural 2025 Magic Quadrant legitimized, and two of the four entries here are its Leaders. The bar was a proven healthcare practice, not a landing page; here is how four intelligent document processing platforms stack up.
11. ABBYY (Vantage / FlexiCapture)
ABBYY provider card: general intelligent document processing, G2 rating 4.5 out of 5 across 364 reviews.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. SOC 2 Type II; enterprise deployment patterns.
Clinical document coverage & accuracy
Strong. CMS-1500/UB-04 claims capture with attachments; referral automation.
Medical language & coding intelligence
Limited. Clinical NLP and code-set inference are not its core.
Fax & multi-channel intake
Strong. Capture across scan, fax, and digital channels.
EHR & interoperability fit
Strong. Capture-to-EHR solutions productized.
Human-in-the-loop QA & exception handling
Strong. Mature validation and review tooling from the FlexiCapture era onward.
Limited. Configuration effort and skills requirement are the recurring review complaints.
Best for
Enterprises with config/IT capacity wanting a claims-forms workhorse
Pricing model
Enterprise / custom
Review signal
G2 ~4.5/5 across 364 seller reviews; Gartner Peer Insights 4.5 across 51 Vantage reviews (re-verify at publish)
The claims-forms workhorse with two decades of capture muscle. ABBYY is a Leader in Gartner’s inaugural 2025 IDP Magic Quadrant, and its healthcare portfolio is concrete: CMS-1500 and UB-04 claims capture with attachments, capture-to-EHR, and referral automation. Review signal is the strongest of the traditional vendors: roughly 4.5/5 on G2 across 364 seller reviews and 4.5 on Gartner Peer Insights for Vantage.
Vendor-published outcomes (80% straight-through referrals, 99% accuracy) are best treated as ceiling numbers, not defaults. Who it’s for: enterprises with configuration and IT capacity that want a proven claims-forms engine. Watch-out: the recurring review complaint is configuration effort and the skills it demands, and clinical NLP is not what it does.
12. Hyperscience
Hyperscience provider card: general intelligent document processing, FedRAMP High authorization achieved December 2024.
Criterion
Grade + evidence
PHI safeguards & compliance
Excellent. FedRAMP High authorization (December 2024).
Clinical document coverage & accuracy
Excellent. Handwriting extraction is the signature strength.
Medical language & coding intelligence
Limited. Claims-document focus, not clinical NLP.
Fax & multi-channel intake
Adequate. Document ingestion, not fax transport.
EHR & interoperability fit
Adequate. Integration-led rather than productized EHR connectors.
Human-in-the-loop QA & exception handling
Strong. Confidence-based routing to human review is central to the platform.
Enterprise and public-sector claims operations with heavy handwriting
Pricing model
Enterprise / custom
Review signal
Gartner Peer Insights 4.4 across 17 reviews; PeerSpot 7.6/10 (re-verify at publish)
Handwriting at public-sector scale. Hyperscience is the MQ Leader positioned furthest for completeness of vision in the 2025 Gartner analysis, holds FedRAMP High authorization (December 2024), and ships a Medicaid claims solution. Its most-cited proof is a federal deployment where a claims backlog dropped from three weeks to about four hours with roughly $46M in annual savings (vendor-published case), and it advertises training on about 400 sample documents (vendor claim).
Who it’s for: enterprise and public-sector claims operations where handwriting volume breaks other tools. Watch-out: entry pricing excludes smaller provider organizations, and the platform’s center of gravity is claims documents more than clinical notes.
A vendor’s 99% accuracy is not your accuracy. Vendor numbers are typically document-level or best-case. Field-level accuracy on your document mix (handwritten, faxed, multi-page) is what decides rework, and human-in-the-loop review remains the real safety net: 90% of denials already receive human review before resubmission (Experian Health, 2025).
13. Nanonets (+ Nanonets Health)
Nanonets provider card: general intelligent document processing, G2 rating 4.7 out of 5 across about 101 reviews.
Criterion
Grade + evidence
PHI safeguards & compliance
Adequate. Healthcare offerings exist; confirm BAA and controls in diligence.
Clinical document coverage & accuracy
Strong. Medical-record automation cases around 50 fields per lab report.
Medical language & coding intelligence
Limited. Horizontal extraction, not code-set intelligence.
Fax & multi-channel intake
Adequate. Email/API/upload channels; fax via integration.
EHR & interoperability fit
Adequate. API-first delivery; EHR write-back is your integration.
Human-in-the-loop QA & exception handling
Adequate. Confidence thresholds with review steps.
Workflow breadth beyond extraction
Adequate. Workflow automations around extraction.
Implementation lift & total cost
Excellent. Published SaaS tiers, usage pricing, fast self-serve setup.
Best for
Mid-size teams wanting self-serve IDP with visible pricing
Pricing model
Published SaaS tiers + usage
Review signal
G2 4.7/5 across ~101 reviews, 86% five-star (accessed July 2026; pin at publish)
The accessible entry point to real IDP. Nanonets holds a 4.7/5 on G2 across roughly 101 reviews (86% five-star, accessed July 2026), with reviewers praising setup speed and OCR accuracy, and it publishes SaaS tiers, which makes it the most accessible starting point in this category. A dedicated Nanonets Health sub-brand now targets SNF and post-acute documentation.
Who it’s for: mid-size teams that want self-serve IDP running this month, with pricing finance can read. Watch-out: it is horizontal-first; the healthcare depth is use-case level, and Nanonets Health is a young sub-brand rather than a hardened clinical stack.
14. Hyland (OnBase + Hyland IDP)
Hyland provider card: general intelligent document processing, G2 rating for OnBase 4.3 out of 5 across 316 reviews.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. Decades of hospital deployment under healthcare controls.
Clinical document coverage & accuracy
Strong. Records classification, referral extraction, billing/coding use cases.
Medical language & coding intelligence
Adequate. Coding-adjacent use cases, not a coding engine.
Fax & multi-channel intake
Strong. Hospital document capture across channels is OnBase’s home turf.
EHR & interoperability fit
Excellent. Deep, long-standing Epic integration.
Human-in-the-loop QA & exception handling
Adequate. Workflow-based review within the ECM suite.
Workflow breadth beyond extraction
Strong. Enterprise content workflow across departments.
Hospitals already on OnBase that want IDP without a new vendor
Pricing model
Enterprise / custom
Review signal
G2: OnBase rates 4.3/5 across 316 reviews; Hyland overall rates 76.8 on KLAS’s latest performance scoring (accessed 2026-07-08)
The incumbent already installed in your hospital. Hyland’s OnBase is widely deployed in health systems with deep Epic integration, and the newer IDP layer adds records classification, referral extraction, prior auth, and billing/coding use cases on top of the content platform hospitals already run. One vendor-published customer case cites a 40% reduction in processing time (PharmaCord; vendor case).
Who it’s for: hospitals already invested in OnBase that want extraction without adding a vendor to the security review queue. Watch-out: it is an ECM-heritage platform, so implementations run heavier, and IDP is a newer layer on a content-management core.
Quick Summary
Q: Which general IDP platforms have real healthcare depth?
A: ABBYY and Hyperscience, both Leaders in Gartner’s first IDP Magic Quadrant (September 2025), for enterprise claims processing; Nanonets for accessible self-serve IDP with a young post-acute sub-brand; and Hyland for OnBase-invested hospital systems. Grade all four on field-level accuracy against your own documents, not their headline numbers.
Best Developer-First Document AI APIs for Healthcare
If your organization has engineers and the goal is extraction inside your own product or pipeline, the platform categories above carry weight you do not need. The developer-first category trades workflow features for healthcare OCR and extraction quality behind an API, and one vendor stands out on healthcare evidence.
15. Reducto
Reducto provider card: developer-first document processing API, field-level page and line citations.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. SOC 2 Type 2, HIPAA, AES-256 at rest and TLS in transit.
Clinical document coverage & accuracy
Strong. Clinical notes, records, forms, and images through one API.
Medical language & coding intelligence
Limited. Extraction-focused; code-set inference is not the product.
Fax & multi-channel intake
N-A. An API: intake channels are your build.
EHR & interoperability fit
N-A. EHR sync is your build.
Human-in-the-loop QA & exception handling
Adequate. Per-field confidence and page/line/region citations feed the review queue you build.
Workflow breadth beyond extraction
Limited. A component, deliberately.
Implementation lift & total cost
Adequate. Usage-based pricing; requires a dev team to amount to anything.
Best for
AI/platform teams embedding healthcare extraction into their own product
Pricing model
Usage-based
Review signal
Formal review volume low; grade on evidence
Extraction as a component, with receipts. Reducto handles clinical notes, records, and forms through one API, and its differentiator maps straight to criteria 1 and 6: field-level citations back to the exact page, line, and region of the source document, which is what an audit-ready extraction layer looks like. Security posture is stated plainly: SOC 2 Type 2, HIPAA, AES-256/TLS.
Who it’s for: AI and platform teams embedding healthcare extraction into their own product. Watch-out: it is a building block, not a workflow; intake, routing, QA staffing, and EHR sync are all still your build, and review-site volume is low, so grade on evidence.
What a modern healthcare document API returns for a faxed referral (illustrative schema, not vendor-specific): typed fields with per-field confidence, so low-confidence values route to human review instead of your EHR.
Q: What is the best document AI API for healthcare developers?
A: Reducto, for field-level extraction with per-field confidence and page/line citations back to the source. It is a component, not a workflow: intake, QA, and EHR write-back stay your build.
Best Cloud Building Blocks If You’re Building It Yourself
One rung below the developer APIs sit the hyperscalers, and the honest framing matters most here: these are HIPAA-eligible building blocks available under a BAA. You are buying materials, not a house. Pipeline, QA, exception handling, and EHR sync are all construction you do. For AWS intelligent document processing and its Google and Azure equivalents, we grade the stack, not the single service.
16. AWS: Textract + Comprehend Medical
AWS provider card: cloud document processing building blocks, ICD-10-CM and RxNorm ontology links via Comprehend Medical.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. HIPAA-eligible services under an AWS BAA; compliance of the workflow is yours.
Clinical document coverage & accuracy
Strong. Textract for OCR, forms, and tables; pre-trained models only.
Medical language & coding intelligence
Strong. Comprehend Medical links clinical entities to ICD-10-CM and RxNorm.
Fax & multi-channel intake
N-A. You build intake.
EHR & interoperability fit
N-A. You build the write-back.
Human-in-the-loop QA & exception handling
Limited. Confidence scores provided; the review system is your build.
Workflow breadth beyond extraction
Limited. Services, not workflows.
Implementation lift & total cost
Limited. Lowest unit cost, highest total ownership; per-page costs compound at volume.
Best for
Engineering teams already on AWS with a data/ML function
Pricing model
Usage (per page / per API call)
Review signal
n/a: cloud services, graded on documentation and reference architectures
The deepest medical building blocks of the three.Amazon Textract handles OCR, forms, and tables (pre-trained only, no custom training), and Amazon Comprehend Medical extracts clinical entities with ICD-10-CM and RxNorm ontology linking, with a published reference architecture for paper-to-electronic claims processing. Three lines of Python turn free-text clinical notes into ICD-10-CM candidates, and that is exactly why this is a building block rather than a pipeline: everything around those three lines is yours to build, secure, and staff.
import boto3
client = boto3.client("comprehendmedical", region_name="us-east-1")
result = client.infer_icd10_cm(
Text="Pt presents with poorly controlled type 2 diabetes and essential hypertension."
)
for entity in result["Entities"]:
top_code = entity["ICD10CMConcepts"][0]
print(f'{entity["Text"]} -> {top_code["Code"]} ({top_code["Score"]:.2f})')
# type 2 diabetes -> E11.65 (0.7x) hypertension -> I10 (0.9x)
Who it’s for: engineering teams already on AWS with a data or ML function. Watch-out: Textract offers no custom training, per-page costs compound at volume, and you own the pipeline, QA, BAA scope, and EHR sync end to end.
17. Google Cloud: Document AI + Healthcare NLP
Google Cloud provider card: cloud document processing building blocks, custom-trained parsers on Google Cloud Platform.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. HIPAA BAA support across the stack.
Clinical document coverage & accuracy
Strong. Document AI custom training plus Gemini-powered few-shot extraction.
Medical language & coding intelligence
Adequate. Healthcare NLP covers medical entities; generic next to specialist medical NLP.
Fax & multi-channel intake
N-A. You build intake.
EHR & interoperability fit
N-A. You build the write-back.
Human-in-the-loop QA & exception handling
Limited. Confidence outputs; review tooling is your build.
Workflow breadth beyond extraction
Limited. Services, not workflows.
Implementation lift & total cost
Limited. Same total-ownership burden as AWS.
Best for
Teams wanting trainable parsers on GCP
Pricing model
Usage
Review signal
n/a: cloud services, graded on documentation
The trainable-parser pick.Google Document AI supports custom-trained parsers and Gemini-powered few-shot extraction, which matters when your document mix includes forms nobody pre-trained for, and the Healthcare NLP API adds medical entity extraction under a BAA. Who it’s for: teams on GCP that want to train parsers to their own documents. Watch-out: the healthcare parsers are generic next to specialist medical NLP; one vendor-published benchmark found specialist medical NLP made 4-6x fewer errors on clinical entities than general cloud APIs (directional, vendor-published).
18. Microsoft Azure: AI Document Intelligence + Text Analytics for Health
Microsoft Azure provider card: cloud document processing building blocks, on-premises container deployment option.
Criterion
Grade + evidence
PHI safeguards & compliance
Strong. BAA support; container deployment for data-residency control.
Clinical document coverage & accuracy
Strong. Custom training plus container/on-prem deployment.
Medical language & coding intelligence
Adequate. Text Analytics for Health covers clinical entities.
Fax & multi-channel intake
N-A. You build intake.
EHR & interoperability fit
N-A. You build the write-back.
Human-in-the-loop QA & exception handling
Limited. Your build.
Workflow breadth beyond extraction
Adequate. Power Automate / Logic Apps ecosystem shortens some paths.
The data-residency differentiator.Azure AI Document Intelligence supports custom training and, distinctively, container-based on-prem deployment, which is the deciding feature for organizations that cannot let documents leave their environment. Text Analytics for Health handles clinical entities, and the Power Automate and Logic Apps ecosystem shortens some workflow paths. Who it’s for: Microsoft-ecosystem organizations and data-residency-sensitive deployments. Watch-out: the build burden is the same as the other two; the ecosystem helps, it does not absolve.
A HIPAA-eligible cloud service is not a HIPAA-compliant workflow. The BAA covers the service. You still own BAA scope, access controls, audit trails, and QA of the pipeline you build on top of it.
Quick Summary
Q: Should you build healthcare document processing on AWS, Google Cloud, or Azure?
A: Only with a real engineering team. Textract plus Comprehend Medical suits AWS-native stacks (no custom training), Google offers trainable parsers, and Azure’s on-prem containers win on data residency. All three are components you assemble, secure, and maintain yourself.
Master Comparison: All 18 Tools on the 8 Healthcare Criteria
Before the decision framework, the whole field on one screen. Find your category first and compare within it; comparing a managed service against a cloud API tells you nothing. The direction of travel is worth naming too: healthcare and life sciences is the fastest-growing IDP vertical, at roughly a 20.95% CAGR through 2031 (Mordor Intelligence, 2025).
~20.95% CAGR through 2031: healthcare and life sciences is the fastest-growing intelligent document processing vertical. Source: Mordor Intelligence, 2025.
Provider
Category
Best for
Pricing model
Review signal
Standout / Watch-out
Forage AI
Managed
Outcome without staffing a platform
Managed service
n/a (graded on evidence)
3x QA, 1-2 week onboarding / not self-serve
Tennr
Fax & intake
Referral-heavy specialty ops
Enterprise
G2: 0 reviews; grade on deployments
~10M docs/month / young, opaque pricing
Medsender
Fax & intake
Clinic fax-to-chart filing
Subscription
G2 sentiment positive; rating not confirmed
EHR filing / SMB ceiling
Documo
Fax & intake
Visible-pricing fax + IDP
Per-page + custom IDP
G2: 4.6/5 (190 reviews)
Published pricing / extraction is add-on
Consensus
Fax & intake
Enterprise HITRUST fax + extraction
Enterprise
No Clarity-specific G2 listing
HITRUST r2 since 2019 / legacy heritage
Waystar (+Iodine)
RCM / PA
Health-system revenue cycle
Enterprise
Best in KLAS 2026, RCM Optimization (98.4)
CDI at scale / suite-only
Infinx
RCM / PA
PA volume, tech + services
Enterprise/services
KLAS 90.1/100 (Apr 2026)
Top KLAS PA score / PA specialist only
AGS Health
RCM / PA
Coding outcomes as a service
Managed services
Best in KLAS 2024, Most Improved Services
Autonomous coding / it’s an outsourcer
Datavant
Abstraction
Network-scale VBC chart work
Enterprise
Best in KLAS 2026, Risk Adj. (90.5)
80K+ facility network / not intake
Reveleer
Abstraction
Focused risk adjustment / HEDIS
Enterprise
KLAS score 75.0; no G2 listing
Focused workbench / payer-side only
ABBYY
General IDP
Claims-forms workhorse
Enterprise
G2 ~4.5/364; PI 4.5/51
Claims capture depth / config effort
Hyperscience
General IDP
Enterprise handwriting volume
Enterprise
PI 4.4/17; PeerSpot 7.6
Handwriting + FedRAMP High / entry price
Nanonets
General IDP
Self-serve, visible pricing
Published SaaS + usage
G2 4.7/~101
Fast setup / healthcare depth is use-case level
Hyland
General IDP
OnBase hospitals
Enterprise
G2 OnBase 4.3/316; KLAS 76.8
Epic integration / ECM-heavy implementation
Reducto
Dev API
Embedding extraction in product
Usage
Low volume; evidence-graded
Page/line citations / component only
AWS
Cloud blocks
AWS-native builders
Usage
n/a
ICD-10/RxNorm linking / no custom training
Google Cloud
Cloud blocks
Trainable parsers on GCP
Usage
n/a
Custom training / generic clinical NLP
Azure
Cloud blocks
Microsoft + data residency
Usage
n/a
On-prem containers / same build burden
Review signals per G2, KLAS, and Gartner Peer Insights, accessed as of July 2026; re-verified at publish.
One caution: this table compresses. The per-item watch-outs above are the real diligence.
Quick Summary
Q: How do the 18 healthcare document processing tools compare at a glance?
A: Category determines fit: managed (Forage AI) vs fax-intake (Tennr, Medsender, Documo, Consensus) vs RCM (Waystar, Infinx, AGS) vs abstraction (Datavant, Reveleer) vs general IDP (ABBYY, Hyperscience, Nanonets, Hyland) vs API (Reducto) vs cloud (AWS, Google, Azure). Pricing runs from published SaaS tiers (Nanonets, Documo) to enterprise-custom everywhere else, and review signals are strongest for ABBYY, Nanonets, and Infinx.
How Do You Choose? Match the Tool to Your Intake Channels and Team Shape
Eighteen graded tools still leave one decision, so here is the tree we would run, keyed to the five intake queues: the fax inbox, the referral desk, the prior-auth desk, claims intake, and records requests. Match the queue first:
Mostly-fax intake (referral desk, records requests): category B. Tennr if referrals drive revenue; Medsender at clinic scale; Documo for visible pricing; Consensus at health-system scale.
Provider-side claims and PA volume: category C. Waystar if you want it inside the revenue cycle; Infinx for PA specifically; AGS if you want the outcome as a service.
Payer-side abstraction and risk adjustment: category D. Datavant at network scale; Reveleer as the focused workbench.
A platform team and multi-department scope: category E, graded on your document mix.
Engineers embedding extraction in a product: category F (Reducto).
Engineers, a cloud commitment, and time: category G, with the build-vs-buy math below.
You want the outcome without the build: category A.
Then gate by team shape. Categories A and B run without engineers. E is for teams with IT and configuration capacity, F and G need a dev team, and C (especially Infinx and AGS) suits organizations comfortable buying part-service. This is where document workflow automation maturity matters more than tool features: hospital documentation software fails on staffing, not capability.
The build-vs-buy honesty box. Hyperscaler APIs carry the lowest unit cost and the highest total ownership: pipeline, QA staffing, BAA plumbing, EHR sync, and permanent maintenance. Buy a platform when your document mix is standard enough for its templates. Go managed when you want SLAs on outcomes instead of a new internal system to run; that is the case the managed category exists for, and the shortest path to test it is a conversation with Forage AI.
Whatever you pick, take the eight criteria into the demo and demand field-level accuracy on your document mix. And if this feels late, it isn’t. The 2025 CAQH Index (released February 2026) found U.S. healthcare avoided $258 billion in administrative costs in 2024 through electronic transactions, with a $21 billion savings opportunity still on the table, and only about 25% of provider organizations using AI in administrative workflows versus 50%+ of health plans (CAQH, 2026). Only 14% of providers use AI in the claims process (Experian Health, 2025). As CAQH CEO Sarah Ahmad put it, “Healthcare leaders are under pressure to reduce administrative costs without disrupting care.” You are not behind. But waiting compounds the backlog.
Forage AI promotional banner reading 10 million-plus documents processed and 95 percent table detection accuracy, with a talk to our expert call to action.
$258 billion avoided, $21 billion still on the table: U.S. healthcare avoided $258B in administrative costs in 2024 through electronic transactions; a $21B savings opportunity remains from full automation. Source: 2025 CAQH Index, released February 2026.
Quick Summary
Q: How do you choose the right healthcare document processing tool?
A: Match the category to your dominant intake queue, then gate by team shape: no engineers means managed or fax-native, a dev team opens APIs and cloud blocks, an RCM appetite points to services. Then pressure-test two or three finalists on the eight criteria with your own document sample.
Expert Insights
“Forcing healthcare providers to change the way they refer their patients doesn’t work. Many have tried. Tennr is the first company that works the way healthcare already does.”
Zeya Yang, Partner, IVP (June 2025). The investor’s thesis doubles as the operator’s selection rule: the winning tool is the one that fits how your intake actually arrives, not the one that asks your clinicians to change behavior.
Frequently Asked Questions
What is healthcare document processing?
Healthcare document processing is the capture, classification, and extraction of structured data from clinical and administrative documents (referrals, claims, notes, lab reports) so downstream systems can act on it. The job is large because an estimated 80% of clinical data is unstructured. It is not document management: DMS stores files, document processing reads them.
How does healthcare document processing software work?
The pipeline runs capture (fax, email, portal, scan), classification and splitting, extraction with per-field confidence scores, validation against rules and code sets, then delivery into the EHR or RCM system. Low-confidence fields route to human review instead of flowing downstream. The write-back step is where most implementations succeed or quietly fail.
Are healthcare document processing tools HIPAA compliant?
Only if a BAA is signed and the workflow around the tool is controlled. “HIPAA-eligible” is not “HIPAA-compliant”: the covered entity still owns BAA scope, access controls, and audit logging. The stakes justify the diligence, with the average U.S. healthcare breach costing $7.42 million in 2025 (IBM).
Why does healthcare still rely on fax?
Interoperability gaps and universal legal acceptance keep fax alive: 35% of inbound documents to healthcare facilities still arrived by fax as of a 2025 industry survey. The modern answer is not ripping fax out; it is extracting structured data from fax automatically so the transport method stops mattering.
How accurate is AI at reading handwritten medical records?
It varies by document mix, and vendor headline numbers are typically document-level or best-case. Handwriting, degraded faxes, and mixed packets pull field-level accuracy below marketing figures. In demos, demand field-level accuracy on your own sample and confirm low-confidence fields route to human review rather than into the chart.
How do you audit automated document processing workflows?
Four instruments: audit trails on every document touch, per-field confidence logs, human-in-the-loop sampling rates, and exception-queue metrics (volume, aging, override rates). If a vendor cannot show you those four in the product, criterion 6 fails, whatever the accuracy slide claims.
Choosing Well in a Market That Won’t Sit Still
Consider how much of this article did not exist a year ago. Waystar closed Iodine in October 2025, Datavant absorbed Apixio and then Aetion, Tennr raised $101M and shipped Voice AI, and Gartner published its first IDP Magic Quadrant ever in September 2025. Every 2025 listicle went stale while its authors slept.
That is the argument for treating a shortlist as a practice, not a purchase. The eight criteria do not churn the way the vendor map does; re-grade your incumbent against them at every renewal, the same way you would grade a challenger. If the incumbent’s watch-out has become your operating reality, that is your signal.
So take the rubric with you. Put your own 40-page fax packet on the table in the next demo, ask for field-level accuracy on it, and ask which fields would have routed to human review. Two or three vendors from this list will handle that conversation well. Those are your finalists, and you will have earned the shortlist rather than inherited someone else’s.
About the Author
Sai S writes about healthcare data and document processing at Forage AI.
Sources
American Medical Association (2026): Prior authorization physician survey, released 2026-05-13 (fielded Dec 2025, n=1,000) · ama-assn.org
Sai is a data infrastructure enthusiast who has spent the past two to three years following the AI space closely, from the infrastructure layer to the fast-growing world of data for AI. He is genuinely curious about how modern data pipelines get built and where the data industry is heading, and he writes insightful pieces on the core topics that shape this niche.